| Stenosis occurs as people
age and the ligaments of the spine thicken and harden,
discs bulge, bones and joints enlarge, and bone spurs
(called osteophytes) form. Spondylolisthesis (the slipping
of one vertebra onto another) can also lead to compression.
The goal of a laminectomy is to relieve pressure on
the spinal cord or spinal nerve by widening the spinal
canal. This is done by removing or trimming the lamina
(roof) of the vertebrae to create more space for the
nerves.
A surgeon may perform a laminectomy with or without
fusing vertebrae or removing part of a disc. Various
devices (like screws or rods) may be used to enhance
the ability to obtain a solid fusion and support unstable
areas of the spine.
Quick Anatomy Lesson
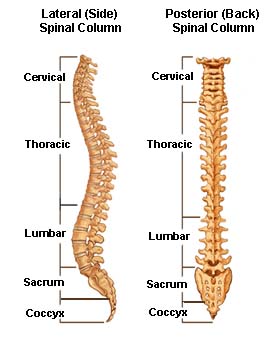
The human spine extends from the skull to the pelvis.
It is made up of individual bones called vertebrae.
The vertebrae, which are stacked on top of each other,
are grouped into four regions:
1) the cervical spine or neck (which is made up of
7 vertebrae)
2) the thoracic spine or chest area (which is made
up of 12 vertebrae)
3) the lumbar spine or low back (which is made up
of 5 vertebrae)
4) the sacrum or pelvis area (which has 5 fused, non-separated
vertebrae)
The base of the spine, the coccyx (or tail bone), includes
partially fused vertebrae and is mobile.
The vertebrae are separated from one another by soft
pads, called intervertebral discs, which allow the spine
to bend and flex and act as shock absorbers during regular
activity. These discs also prevent the vertebrae from
rubbing against each other. Each disc is made up of
two parts, a soft center called the nucleus and a tough
outer band called the annulus.
Throughout the length of the spine is a central tube,
surrounded by bone and discs, called the spinal canal.
Inside the spinal canal are the spinal cord, the cauda
equina, and spinal nerves. The spinal cord begins at
the base of the brain and ends in the lumbar spine area
in a bundle of nerves known as the cauda equina. A pair
of spinal nerves branch out (one to the left and one
to the right) at each vertebral level. These provide
sensation and movement to all parts of the body. A lumbar
laminectomy may be necessary to relieve pressure on
the spinal canal.
Part 2: The Procedure
How the Procedure is Done
The patient is usually positioned face down on an operating
frame. A small incision (usually about 3-4 inches, though
it may be longer depending on how many levels of the
spine are affected) is made in the lower back.
The surgeon uses a retractor to spread apart the muscles
and fatty tissue of the spine and exposes the lamina.
A portion of the lamina is removed to uncover the ligamentum
flavum - an elastic ligament that helps connect two
vertebrae.
Next an opening is cut in the ligamentum flavum in
order to reach the spinal canal. Once the compressed
nerve can be seen, the cause of compression can be identified.
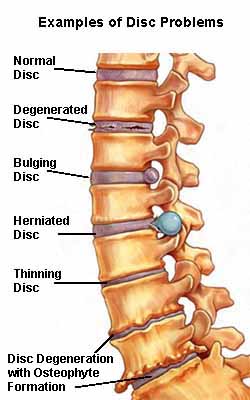
Most cases of spinal compression are caused by a herniated
disc. However, other sources of pressure that can cause
compression may include:
1 - A disc fragment (this will often cause more severe
symptoms)
2 - An osteophyte or bone spur (a rough protrusion
of bone)
3 - Protruding/degenerating discs
4 - Facet arthritis and/or cysts
5 - TumorsThe surgeon retracts the compressed nerve
and the source of the compression is removed and pressure
on the spinal nerve or nerve components is relieved.
If necessary, the surgeon will perform a spinal fusion
with instrumentation to help stabilize the spine. This
occurs when a lot of bone needs to be removed and/or
when multiple levels are operated on. A spinal fusion
involves grafting a small piece of bone (usually taken
from the patient's own pelvis) onto the spine and using
spinal hardware, such as screws and rods, to support
the spine and provide stability.
Then the procedure is finished! The surgeon will close
the incision either using absorbable sutures (stitches),
which absorb on their own and do not need to be removed,
or skin sutures, which will have to be removed by the
surgeon after the incision has healed.
|



 Vincent
Traynelis, M.D.
Vincent
Traynelis, M.D.